May 2, 2023

CHICAGO — When internal medicine physician David Ansell started his career in 1978 at “County,” the sprawling public hospital that treated many of this city’s poorest residents, he didn’t question why so many of them were so sick, and their cases so complicated. “I just thought these were conditions they just had,” he said in a recent interview.
Ansell, then 27, went on to work for nearly two decades at Cook County Hospital and then spent a decade at nearby Mount Sinai, which also serves the economically distressed West Side neighborhoods that surround it. His patients flowed in with hypertension, diabetes, kidney disease, and joint pain. He did the best he could with the resources he had.
From his ninth-floor corner office, Ansell could see two aging and empty towers: the old Sears Roebuck Company headquarters that closed when the company moved to its namesake skyscraper in Chicago’s Loop, and the long-shuttered Western Electric Plant, which had once employed 25,000 people making telephone equipment. For Ansell, the connection between the white flight and loss of businesses from these once thriving neighborhoods and the poor health of the residents who remained was starting to become clear.
It wasn’t until Ansell started working at Rush University Medical Center that it all clicked. Rush is in the same area, but provides costly specialty care of all kinds and largely serves patients with private insurance. Ansell had never seen one of his County patients get a joint replacement; the wait list is about five years. At Rush, patients can receive a new hip within weeks. The busy trauma centers at County and Mount Sinai harvest a large number of organs for transplant surgeries done elsewhere including Rush; none of Ansell’s County patients had ever received a transplant.
He was seeing, he now understood, two different Americas, and two very different health care delivery systems. This was why his Cook County Hospital patients had always been so sick while his Rush patients seemed as though they “had landed on another planet,” one where they could miraculously live so much longer.
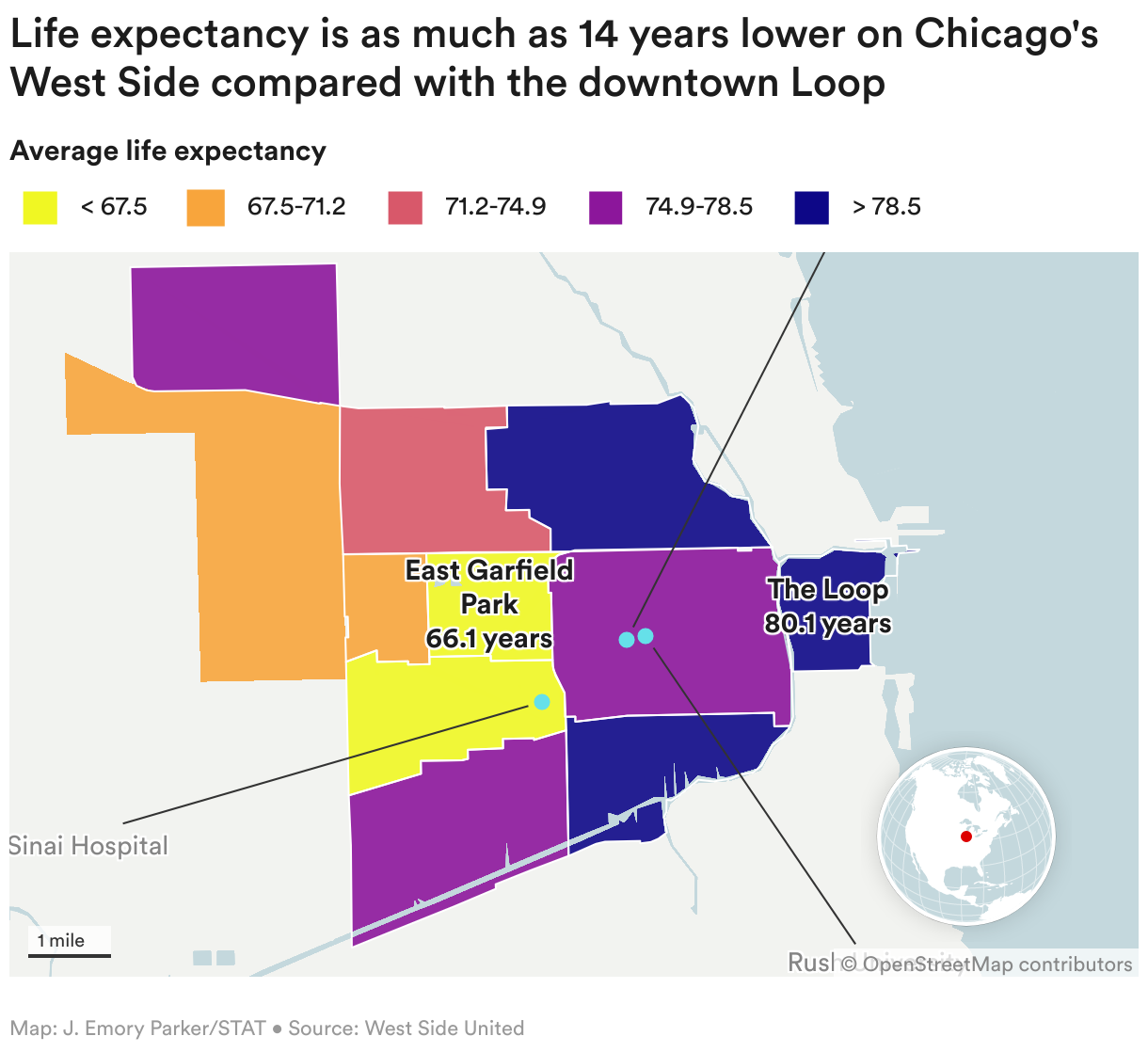
The revelation of this “death gap” spurred Ansell to look more closely at the neighborhoods around his hospital, and to visit many of them for the first time. He found people living in the East Garfield Park neighborhood near Rush lived 66 years, on average, 14 years less than residents of Chicago’s Loop just a few miles away. But Ansell didn’t know what to do about it. In medical school, he’d learned to treat heart disease and diabetes. He hadn’t learned how to treat inequality.
As Rush’s chief medical officer, he’d spent 10 years focused on improving quality and making sure his hospital did not harm the patients that entered. But none of that work, he realized, was closing the life expectancy gap that yawned just outside his hospital’s walls. To do so, Rush would have to do something it had never done before: Instead of focusing only on health, it would have to focus on wealth. The hospital’s anchor project was born.

Anchor projects have been around for decades, often started by universities hoping to help revitalize their distressed surroundings. These “anchor eds,” as they are called, can’t easily uproot because of their large and entrenched physical footprints; think Yale or the University of Southern California.
Hospitals, or “anchor meds,” came to the game much later, urged to use their clout to curb health disparities by the National Academies of Science, Engineering, and Medicine in 2017, and spurred by Affordable Care Act rules requiring community needs assessments. Rush’s work was already underway.
Ansell had gone to his board in 2016 with a chart demonstrating how much earlier people who lived in neighborhoods around Rush died, compared with the city’s wealthier and whiter neighborhoods. The board was shocked by the actual numbers, he said, and agreed to embark on a strategy to address the great need outside their doors.
The health system changed its mission from being best in patient care to improving the health of the diverse communities it serves and made equity one of its critical strategies. Rush leaders also publicly stated — long before the racial disparities in pandemic deaths and police violence of 2020 highlighted the issue for many others — that structural racism and economic deprivation were the root causes of many health disparities.
“That was huge for us to hear someone acknowledge it,” said Redia Holman, a patient care navigator at Rush and Black West Side resident who co-authored a recent New England Journal of Medicine article on Rush’s anchor project with Ansell. “It shifted some trust.”
The project started in 2017 with what Ansell calls the “first community” — Rush employees who live on Chicago’s West Side. Many of those workers are the health system’s lowest earners and are Black and female. An analysis showed they were less likely to save for retirement and more likely to be in financial distress.
No one liked what they saw. “It was not our intention to have people who work for us live in poverty,” Ansell said. Executives set about increasing wages and finding ways for more employees to save for retirement. The number taking full advantage of Rush’s retirement match program jumped from 34% in 2017 to nearly 80% in 2021.
Addressing in-house issues helped the reality of the wealth gap hit home, Ansell said. “You take a big idea like structural racism which can be hard to grasp, but we said, ‘Hey, these are people we know,’” he said. “That’s Hank in transport, that’s Evelyn in the E.D.”
Next in the effort to address the area’s needs was a listening tour to find out what the community needed. Rush had been on Chicago’s West Side for 180 years — its charter preceded the city’s by two days — but over the years, the institution lost credibility with many who lived nearby, Ansell said.
What residents told Rush leaders was eye-opening, and sometimes hard to hear. Many folks were angry. They complained that hospitals kept making promises they couldn’t keep, or giving out grants that lasted a year or two before everything went back to the way it was before. Community members said they wanted well-paying jobs that led to careers. They wanted safe places where they could walk and children could play. They wanted more local businesses and grocery stories with fresh produce.
One thing they didn’t ask for? More clinics. “No one wanted more health care,” Ansell said.
The West Side of Chicago is expansive, with some 500,000 residents. The Rush team realized the problem was bigger than them. So in 2018, Ansell asked other area hospitals to join. Six did, as did many representatives from the community. The group is known as West Side United.
As the work was progressing, Ansell got a call from the American Medical Association, the physician trade group that had long leaned conservative — and that the progressive Ansell had vowed never to join. Some of its executives wanted him to come in to discuss his book, “The Death Gap.”
“I feel like I’m Moses walking into the Pharaoh’s palace,” Ansell recalled of walking into the AMA’s opulent downtown Chicago headquarters. Ansell challenged the AMA to join West Side United. The association did, and has since contributed $5 million. Ansell, in turn, became an AMA member. “It was the least I could do,” he said.
West Side United brought in community activist Ayesha Jaco to run the organization in 2018. For Jaco, the life expectancy gap hit close to home. She had lost her grandmother, just two weeks after she was diagnosed, to ovarian cancer at age 66. She warned the hospitals that community members, who’d been let down countless times and were tired of promises, would be watching closely. “There’s a lot of fatigue,” she said.
Work was well underway to analyze the community’s needs, start collecting data on health outcomes, and to map the area’s many assets — grassy parks, historic architecture, vibrant churches, and long-time small businesses. Then Covid hit.
Rush was uniquely positioned to respond: Its 14-story tower was designed shortly after 9/11 with separate triage bays and negative-pressure air systems specifically to handle pandemics and mass casualty events. The hospital took in some of the city’s sickest Covid patients. Rush, Ansell proudly reports, had some of the lowest Covid-19 death rates in the nation, and unlike many other hospitals, did not see far higher death rates in Black and brown patients.
But the grim reality of Covid means that during the pandemic, the life-expectancy gap in Chicago that West Side United pledged to cut has now risen by more than two years.

Cesar Torres is zooming around on a cherry picker, grasping boxes of syringes, lidocaine, and Post-its — anything a hospital might need. He’s an employee, one of many who live nearby, at the West Side warehouse that supplies local hospitals with most everything they need, from medicines to wheelchairs. In thinking through how Rush might spur economic development in the neighborhood, leaders realized the hospital’s supply chain was a powerful tool.
In 2018, as Rush looked to update its obsolete medical supply warehouse, it partnered with Ohio-based medical supply distributor Concordance Healthcare Solutions, whose leaders agreed to retain the 30 current warehouse employees and hire new workers from West Side neighborhoods.
Concordance built a 175,000 square foot high-tech warehouse in the Little Village neighborhood that could employ nearly 80 because it serves other hospitals as well. Not only is the gleaming new building a boost to the neighborhood, the increased efficiency of the warehouse saves Rush $1 million a year, money that Rush CEO Omar Lateef says allows the hospital “to reinvest even more into the community.”
The project is going so well, said James Knight, a region director for Concordance, the company hopes to replicate it with willing hospital partners in other areas. “This format of creating jobs and opportunity is easily duplicated, and not just on the West Side of Chicago,” he said. “It can be on the South Side. It can be in LA or New York. ”

It’s been a boon for employees like Torres, who after a series of mainly temporary jobs, has worked here three years and is on an upward career trajectory. “I’ve been in other warehouses, but they never pushed me to learn,” he said. “This is one of the first stable jobs I’ve had.”
Joel Jaffe, a Concordance account manager, grew up nearby but moved away as a child and is thrilled to be back making a difference for so many families. “You’re literally touching an entire community,” he said.
In addition to the warehouse, and providing area residents career pathways into higher paying medical jobs, West Side United hospital systems contribute millions in funding for “impact investments.” Through local community development institutions, the money flows to businesses and projects like the Hatchery, which offers “life and knife skills” classes to train residents for jobs in Chicago’s high-end restaurants. It also rents kitchen space to food industry entrepreneurs like Eudell Watts II, allowing him to grow his Old Arthur’s barbecue sauce and dry rub business, using family recipes from his once-enslaved great, great grandfather.
Another recipient, Circle Urban Ministries, used an $800,000 low-interest loan to build a 12-unit apartment building with childcare for women in drug recovery who want to keep their families intact. Getting such funding, the organization’s CEO James Borishade said, had been nearly impossible due to barriers he faced from traditional banks. Now, he’s at work on a new project to build more transitional housing and run a financial education program to put recovered mothers on a path toward home ownership and increased family wealth.
And that original $800,000 loan that commercial banks thought was too risky to lend him? “I’m pleased to report,” Borishade said, “we’re fully paid back.”

Hospitals still have a long way to go. A recent analysis by the Lown Institute, a health care think tank, found that more than three-quarters of nonprofit hospitals spent less on charity care and community investment than they reaped in tax breaks. But a national collaborative called the Healthcare Anchor Network, with more than 70 health systems, is trying to do more. Together, the group is an economic powerhouse, spending $150 billion each year, employing 2 million people, and holding $500 billion in investment portfolios.
“Moving just 1% of hospital investments into community projects can make a huge difference,” said the network’s president and founder, David Zuckerman. “We tell them don’t just be your ivory tower … think about being an economic engine.”
One system that’s embraced that idea is BJC Healthcare, the largest employer in the state of Missouri. It’s based in St. Louis, where health and wealth gaps mirror those in Chicago. Anchor initiatives there are headed by Christopher Nolan, who worked at Rush for eight years before moving to BJC.
He’s been busy. The health system partnered with St. Louis-based community development organization Beyond Housing to build a slew of new affordable family homes, backed initiatives to provide low-interest loans to Black- and Hispanic-owned businesses and help residents refinance predatory car loans, and supported two local Black-owned or managed banks that make community loans.
One loan went to Freddie Lee James Jr., who said trying to get a conventional loan for his gourmet-sauce business had been a “nightmare,” despite having a good credit score and little debt. With the new loan, he’s hired more workers and opened a larger bottling facility last month, which supplies sauce to thousands of stores and bottles sauces for other entrepreneurial hopefuls.
Nolan said the anchor projects are happening because leaders at his organization, from the CEO to the treasurer, see and understand the work as investments that help both the health system’s bottom line and the health of the community. “It’s aligning our investments with our mission,” Nolan said. “It doesn’t have to be one or another.”

It’s not just big hospitals and health systems that are getting involved. In Atlanta, a group of federally qualified health clinics called Mercy Care has launched a $50 million project to build 170 apartments — a mix of subsidized and market-rate units — on land adjacent to one clinic in the Sweet Auburn neighborhood.
The birthplace of Martin Luther King Jr., the historic downtown neighborhood has become gentrified: Many clinic staff can no longer afford to live nearby and many of the patients — 75% who live below the federal poverty line and half of whom are unhoused — struggle to do so as well.

The new building, expected to open next year, will include transitional housing and permanent housing with support services set aside for patients who have long been unhoused. “It’s going to be beautiful. It has a rooftop deck, just like you might find in any of the more expensive properties nearby,” said Kathryn Lawler, chief executive of Mercy Care and its parent company the St. Joseph’s Health System, which is a member of national Catholic health system Trinity Health.
The project is a good fit for Mercy Care, which has its roots in the Sisters of Mercy, nuns from Ireland who showed up in Atlanta, opened the city’s first hospital, and, realizing the connection between health and housing, also opened a nonprofit called Mercy Housing. But Lawler said non-faith based health systems can play a role as well. “Everybody owns land, everybody’s in the construction business, hospitals do this all the time, you really can participate,” she said.
Many health executives, said Lawler, remain timid, and a little bit afraid, about taking on social issues outside of medicine. “They think if you do housing, the next thing is you’re going to have to solve the war in Ukraine,” she said. “That’s not going to happen.”
What Rush needs to do now is show that the community development effort is indeed improving health outcomes, and extending life spans in the 10 neighborhoods it is helping to revitalize. “What was an audacious goal before Covid is even more audacious now,” said West Side United leader Jaco.
The work is a long game. While studies show providing housing saves money by reducing hospitalizations, and new research, including a study published just last month, ties shorter life spans to living in less advantaged neighborhoods, project leaders know it could take decades to show the improvements they are making lead to better health and longer lives. Collecting data is key to the project, said Rukiya Curvey Johnson, Rush’s vice president for community health equity and engagement. West Side United is tracking dozens of metrics of both neighborhood and health improvement against its stated goals on a public dashboard. “It helps the public hold us accountable,” she said. “More importantly, it helps us hold ourselves accountable.”
Curvey Johnson acknowledges that even making a dent in these numbers is a daunting task. On a recent tour of some of the neighborhoods here, with some streets speckled with trash, vacant lots, and boarded up storefronts, she said health systems like hers have to stop “gazing at the problem” and just get to work.
“It can seem overwhelming, like there’s nothing we can do, but you have to start somewhere,” she said. “We’re the biggest employer on the West Side, we’ve been here since the founding of Chicago and we’re not going anywhere. How can we leverage that?”
This is part of a series of articles exploring racism in health and medicine that is funded by a grant from the Commonwealth Fund.
About the Author
To submit a correction request, please visit our Contact Us page.





STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect