Blog


 Reid Porter
Reid Porter340B markup program is a hidden tax, increasing costs for employers, straining state and federal budgets

A tranche of recent reports reveal that the 340B hospital markup program is costing states and the federal government hundreds of millions of dollars in lost tax revenue.
This little-known federal program allows big tax-exempt hospitals and clinics to buy medicines at below-market rates and mark them up to health plans and patients. As a result, it’s a hidden tax on patients, employers and taxpayers.
Three new studies highlight how the 340B markup program is increasing costs on taxpayers.
-
State health plans often don’t receive negotiated manufacturer rebates when hospitals, and their contracted for-profit pharmacies, dispense medicines purchased at the 340B price to state employees. This loss of savings results in increased costs to cover employees, which leads to higher premiums and increased out-of-pocket burden on employees.
Proposed Utah S.B. 69, which would expand the use of 340B contract pharmacies, underwent a cost assessment which reveals it would cost the state significantly while benefitting large tax-exempt hospitals, not patients. The expansion would result in nearly $4 million lost in drug manufacturer rebates for the state employee health plan and could add at least $1.9 million to the state budget. This is because the bill would allow hospitals to further expand their use of for-profit pharmacies, which have little connection to 340B’s original safety-net mission. Instead of helping patients, this expansion would fuel an even greater number of hospital medicine markups, increasing state costs without delivering meaningful benefits to those the program was meant to serve.
These excessive costs are possible across the country and difficult to justify as state budgets are increasingly strained.
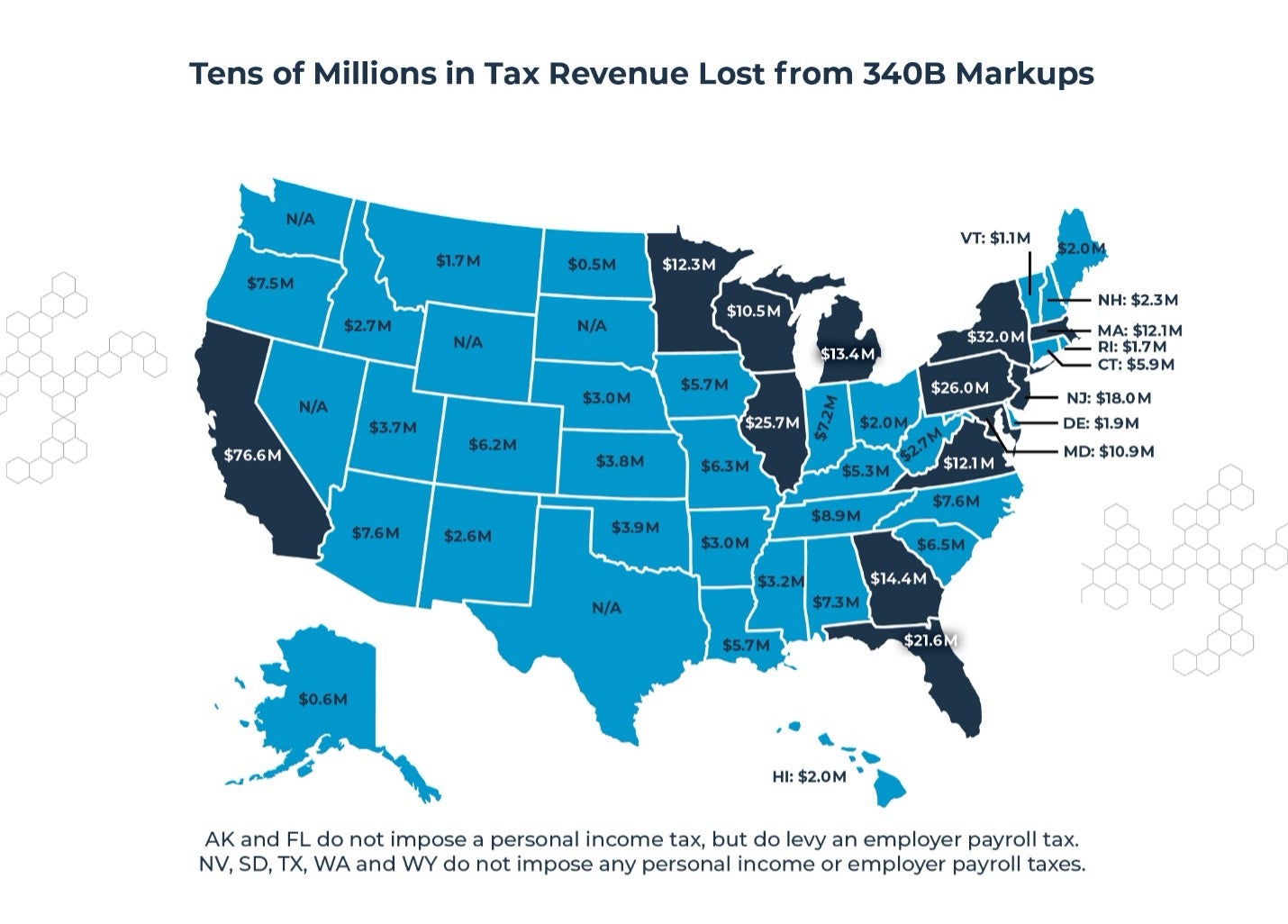
- Federal tax revenue fell by $1.4 billion and state and local taxes by $400 million in 2021 due to employers paying more than they should for medicines purchased at the 340B price, according to a Magnolia Market Access report. When employers are forced to spend more on inflated health care costs, they divert funds away from taxable wages and profits into non-taxable health care expenses. As a result, billions in potential tax revenue are lost each year, while tax-exempt hospitals and for-profit middlemen pocket these profits. This costly system not only burdens employers and workers but also weakens public funding for essential services.
- Lost rebates on prescriptions filled in 340B increased employer health care costs by more than $6.6 billion, and state and local government plans by more than $1 billion in 2023 according to IQVIA. 340B contract pharmacy mandate bills would further increase this cost by $1.9 billion for employers and $273 million for state and local government health plans.
- 340B warps local health care markets by incentivizing consolidation, a phenomenon that is responsible for up to $32 billion per year in additional Medicaid spending, according to Health Capital Group. Analyses have found Medicaid spending rises most quickly in regions that see high 340B growth and health care consolidation, which leads to increased hospital market power, higher prices, and shifting patients to more-expensive sites of care.
North Carolina was one of the first states to sound the alarm in 2024, finding that 340B hospitals are charging the state five times what they pay for 340B medicines, a conclusion bolstered by a New England Journal of Medicine study. And the evidence that 340B hospitals are failing to invest in charity care continues to mount, with research showing that nearly all 340B hospitals make more from 340B than they invest in charity care.
Given this recent data, it's little wonder that cash-strapped governments are beginning to question the 340B model, in which marked up medicines drive hospital, clinic, and for-profit pharmacy profits without any data suggesting that those profits find their way back to vulnerable patients or rural communities in the form of more affordable, more accessible medicines.
