
Understand how science, health policy, and medicine shape the world everyday. Sign up for our Morning Rounds newsletter here.
Good morning. Reproductive health is dominating the news and the newsletter this morning. We also have a look at the decade-long battle over a patent for CRISPR. It’s been a rollicking ride.
Supreme Court to hear case on medication abortion
The U.S. Supreme Court said yesterday it will hear a case challenging Americans’ access to a pill commonly used in abortion that could also potentially limit the FDA’s regulatory powers. In what will be the high court’s first major abortion case since it overturned Roe last year, it will consider state restrictions on mifepristone, a pill approved by the FDA more than 20 years ago. Used with another drug, misoprostol, it is approved for abortions up to 10 weeks, when most abortions take place. Medication abortions account for roughly half of procedures each year.
How did we get here? A conservative Texas judge ruled in April that the FDA “acquiesced on its legitimate safety concerns” amid political pressure to approve the drug. The same day, a Washington state judge ordered the FDA to maintain its approval and drop prescribing restrictions because it had been proven safe over years of use. STAT’s Sarah Owermohle has more.
When Dobbs forced one doctor to shutter his abortion clinic, he took his mission on the road
When the Supreme Court’s Dobbs decision overturned the constitutional right to an abortion in the U.S., it also upended the life of Aaron Campbell (above), who on that day in June 2022 turned away a patient seeking abortion for the first time. Lawyers at his clinic, the Knoxville Center for Reproductive Health in Knoxville, Tenn., urged him to stop performing the procedures immediately in the uncertain medical and legal atmosphere.
Instead of moving to another state, Campbell has become a traveling abortion provider, going from clinic to clinic, state to state, license by license. Inspired by his father’s career in the same clinic, he sees his role this way: “I want to help this person with what they think is best for themselves, and all of us know ourselves better than anyone else,” he said. “Everyone probably knows someone who’s had an abortion.” STAT contributor Amy Pedulla has more.
Teen pregnancies down, but remain higher in the U.S.
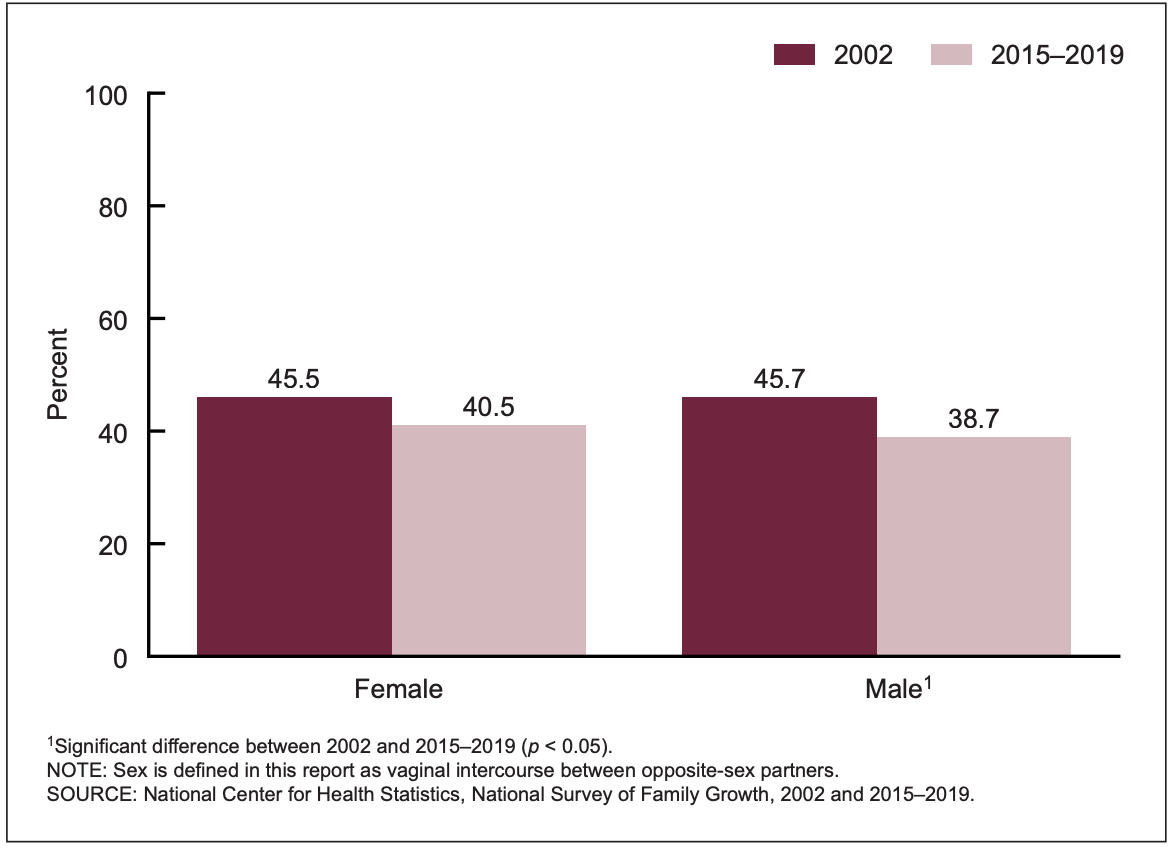
Reproductive health has been in the spotlight since the U.S. Supreme Court’s Dobbs decision last year and will likely stay there with yesterday’s news on mifepsritone, meaning a renewed focus on contraception when abortion access is not certain. A new CDC report updates its survey of U.S. teenagers’ sexual activity, zeroing in on intercourse, contraceptive use, and childbearing. Teen pregnancy and birth rates and pregnancies have continued to decline since the 1990s, but that new low is still almost twice as high as rates recorded in Canada. This chart compares the percentage of unmarried 15- to 19-year-olds who had never had sex in 2002 versus 2015-2019:
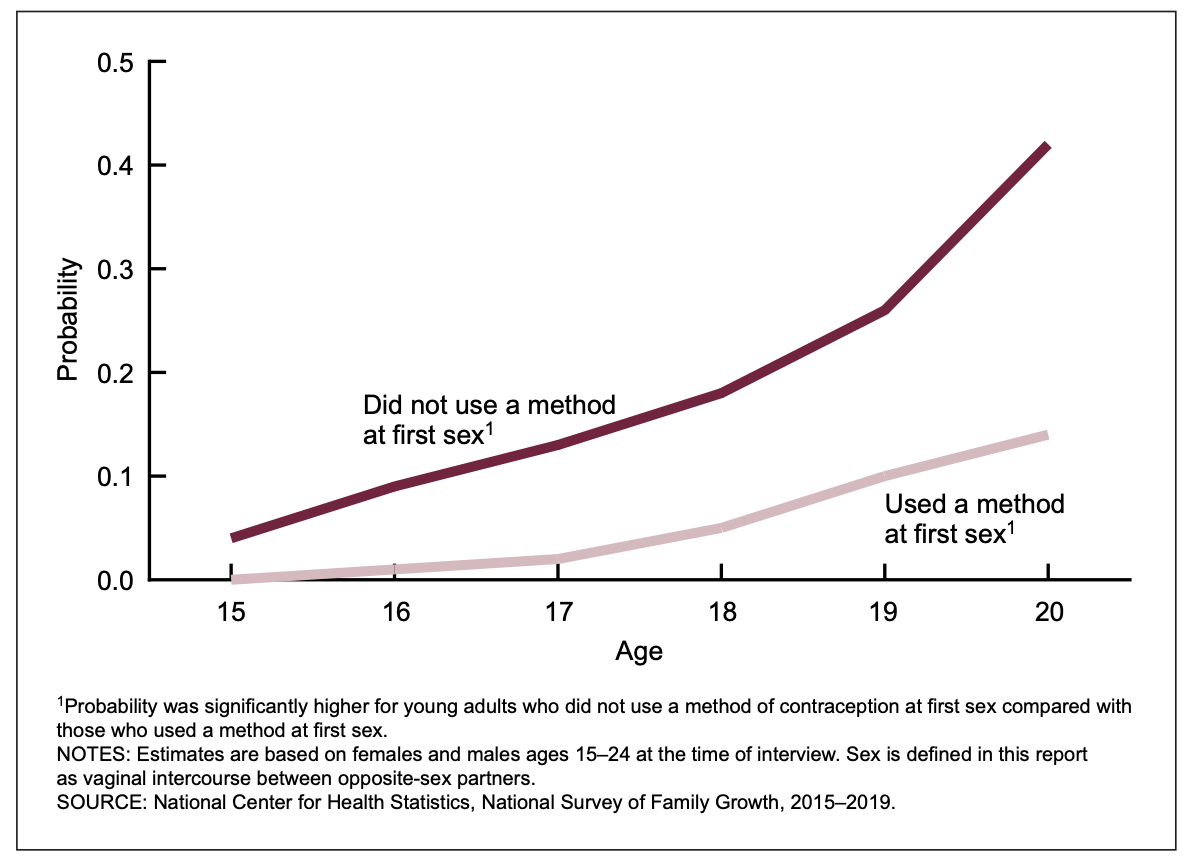
And this one shows the probability of having a first birth and whether protection was used:
Another twist in the CRISPR patent tale
You could say George Church called it. Yesterday marked another chapter in how the patent-right story has evolved around the revolutionary genome editing tool CRISPR-Cas9. Vertex Pharmaceuticals — fresh from its newly approved sickle cell therapy based on CRISPR — said yesterday it will pay Editas for rights to use in Casgevy.
Before settling into business as usual, a dispute arose when Editas was spun off from Harvard and the Broad Institute, where Feng Zhang had done some of the first work showing CRISPR could work in human cells. Two other companies — CRISPR Therapeutics (now Vertex’s partner on Casgevy) and Intellia got their licenses from University of California, Berkeley, and the University of Vienna, where future Nobel laureates Emmanuelle Charpentier and Jennifer Doudna led the earliest work showing CRISPR could edit genes in a test tube. Church, Doudna, and Zhang started Editas, and Doudna and Church have been involved in Intellia.
“There’s plenty of different ideas and companies to go around,” Church said on the day in 2020 Doudna and Charpentier got their Nobel call. (“Definitely they made the key discovery, which was that you … can program an enzyme, Cas9, to cleave at a particular place in DNA,” he said then.) “In fact, if anything, there’s not enough patents. Not enough companies.” STAT’s Jason Mast has more on what yesterday’s win means for Editas.
A clue to nausea and sickness in pregnancy
“Morning sickness” is such a mild-sounding name for what can be torment. More than two-thirds of pregnant mothers experience nausea and vomiting, but a fraction are so severely ill they must be admitted to hospitals to get IV fluids for dehydration. New research in Nature finds a connection between levels of a hormone during pregnancy and such serious illness, but not in a simple way.
The “what” was already known: a hormone called growth differentiation factor 15. The “how” was not. It turns out the fetal part of the placenta produces high levels of this hormone, which causes trouble if the mother had low levels before becoming pregnant. That fits with previous research showing women with beta-thalassemia, who always have high levels of the hormone, rarely have nausea and vomiting in pregnancy. Understanding this inverse relationship — low levels before, high sensitivity later — might lead to treatments, the authors suggest.
Hospital records don’t always show when a patient has died
Health professor Neil Wenger was deep into a years-long study on seriously ill primary care patients when he uncovered a different but persistent issue: Many patients who were targeted for follow-up interventions had actually died, and their hospitals did not know about it.
That’s a problem for multiple reasons, including the fact that incomplete patient data could seriously impair health systems’ charge toward AI and predictive algorithms. Wenger and a team of researchers are now leading the effort to get health systems to update their verification process and pressuring legislators to make death data more accessible. Read more from my colleague Mohana Ravindranath.
About the Author Reprints
To submit a correction request, please visit our Contact Us page.











STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect