
While much of the health care workforce is battling staff shortages, the emergency medicine field is trying to figure out how to manage a potential oversupply of physicians.
The American College of Emergency Physicians predicted in a 2021 study that there would be a surplus of nearly 8,000 emergency physicians by 2030.
In the wake of this news, medical students’ interest in the field nosedived over the next two years. Whereas 99.5% of emergency medicine residency positions were filled in 2021, there were hundreds of unmatched seats in emergency medicine residencies in 2022 and 2023 — 554 of them this year alone.
Citing the excess of emergency residency spots — along with financial concerns — Christus Spohn Hospital in Corpus Christi, Texas, announced on Oct. 12 plans to shut down its entire emergency residency program. The decision has alarmed doctors and patients across Corpus Christi and Texas, who note that it’s the only emergency medicine residency in South Texas, potentially cutting off an underserved community from a pipeline of much-needed doctors.
Experts told STAT that it’s possible that emergency medicine residencies may have to close, or at least shrink, in order to make better use of the available resources for graduate medical education. But they also say there are far better ways to address worries over a surplus — which may not even wind up coming to pass, given the pandemic and other factors — such as cutting down on new residency program approvals and expansions.
The situation in Corpus Christi shows how complex it will be to fix the country’s inefficient medical residency system, which is ruled by outdated government stipulations regarding how many slots the government will fund and how much it will pay per resident. Emergency physicians are also worried that the current system lets corporate interests warp the residency landscape and make the workforce problem worse, to the detriment of doctors, future doctors, and patients.
“There needs to be a national collaborative approach towards the physician workforce in a way that would guarantee more equitable funding in terms of geographical distribution, but also funding in terms of what specialties we actually need more people of and which ones we don’t,” said Blake Denley, an attending physician at Ochsner Health in New Orleans and president of the Emergency Medicine Residents’ Association. “Essentially, no one is making those decisions.”
What’s affecting the supply of emergency physicians
The 2021 ACEP study warning about a bleak future job market for emergency physicians led some deans and advisors to dissuade medical students from pursuing careers in the field, according to a report earlier this year from the Emergency Medicine Residents’ Association. But there may not have ever been such a large, looming surplus in the first place.
The ACEP study, which began in 2019, made a number of assumptions based on available data at the time. It predicted the demand for emergency physicians would decrease over the ensuing decade because the number of physician’s assistants and nurse practitioners practicing in the ER had risen by an average of 8.9% every year over the previous seven years. It also assumed that the number of emergency physicians graduating from residency would increase by 2% every year, and the workforce would see 3% attrition each year.
But ACEP president Aisha Terry told STAT that those attrition rates may not be valid in the post-pandemic landscape. A recent study showed that the attrition rate for board-certified emergency physicians was as high as 7.6% in 2020, which the study did not take into account.
The study was a snapshot in time, she explained: “The variables that we’re now working with have actually changed, which then of course changes the entire formula, if you will, and then ultimately would impact the ultimate prediction in terms of workforce.”
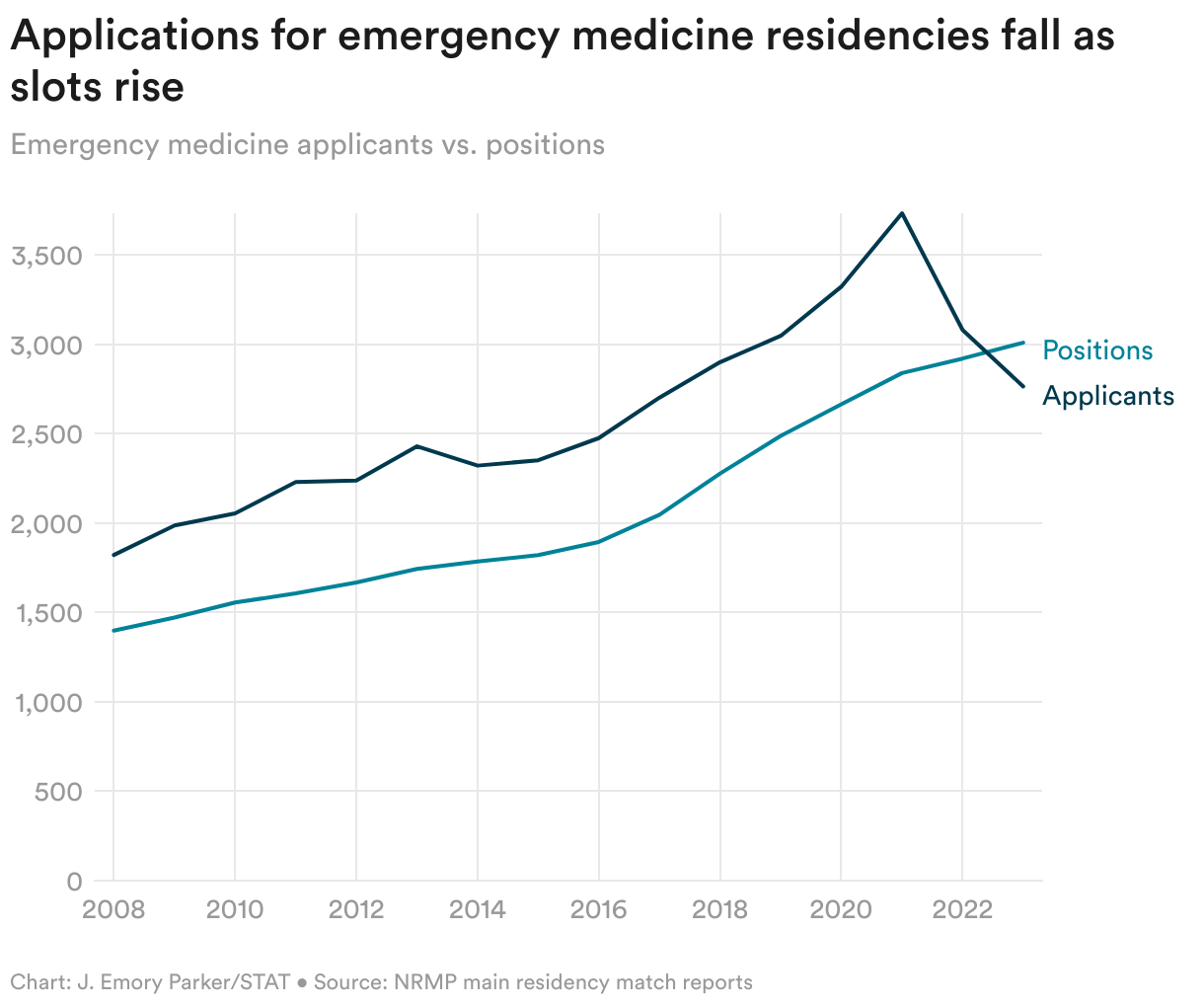
While interest in the field has plunged, the number of available residency spots is still rising — not necessarily because of demand, but for financial reasons.
“A big concern within emergency medicine right now is private equity’s involvement within medicine, but also within the training of residents,” said Denley of the EMRA.
Residents are paid less than not only their attending physician counterparts, but also less than the nurse practitioners and physician’s assistants now staffing emergency rooms. Many are concerned that because of this, some health care systems have opened residency programs motivated less by education than by the opportunity for cheap labor, Denley and other experts told STAT.
No party in the convoluted medical residency governance structure actually controls the total number of residency spots, how they’re spread out across different specialties, or how they’re geographically distributed. While the Centers for Medicare and Medicaid Services funds many residency spots and has tried to influence some of those factors, any institution that wants to open a residency program can do so if it decides to fund the program itself.
The body that approves residency programs, the Accreditation Council for Graduate Medical Education, can only give a “yes/no” answer on whether programs meet quality standards for medical education. It doesn’t render judgment on programs based on workforce needs or financial factors.
Many people have told ACGME, “‘Stop accrediting these programs. We don’t need any more in this area,’” said Denley. “But they don’t have the power to do that.”
The Christus emergency medicine residency closure
When hospital administrators told faculty and residents at the Christus Health-Texas A&M Spohn emergency medicine residency earlier this month that the program was going to shut down, they explained that its resources would be moved to the family medicine program, a Christus employee told STAT. Each of the program’s current 36 residents are welcome to stay and graduate, said officials, but the program will stop operating in spring 2026, when the current intern class graduates.
“It is not common at all” for an emergency residency to close down like this, said Sandra Williams, president of the Texas College of Emergency Physicians. She could only think of two examples of emergency programs shutting down: Hahnemann University Hospital in Philadelphia, which declared bankruptcy in 2019, and the University of Texas Medical Branch in Galveston, where Williams works, which got hit by Hurricane Ike in 2008.
“But this is the first I’m aware of a program being closed down while the hospital still exists and continues,” she said.
Faculty and residents were blindsided by the decision. Christus first told them, and STAT, that the closure was for financial reasons.
The decision “was made with thorough consideration of our community’s needs and our ministry’s available resources to serve those needs. We ultimately determined that our ability to sustain this program would end with graduating this cohort in 2026,” it said in a statement.
After further questions, the hospital sent STAT an expanded statement citing the “national oversupply of emergency residency slots” and the emergency medicine physician surplus as an additional reason for the closure.
Christus promised that the quality of care at its hospitals will not change with the end of its residency program. Community leaders, however, are concerned. “This will affect the quality of care. There is no question about it in anybody’s mind, respectfully, but Spohn’s,” said Corpus Christi city commissioner Brent Chesney, speaking to the Nueces County Hospital District board at a meeting on Oct. 24.
To keep up the current level of care without residents will be expensive: Three emergency medicine residents currently run the entire trauma ICU 24 hours a day, seven days a week. The 36 residents in the program also work in the medical ICU, labor and delivery at a different Christus hospital, the pediatric ICU and emergency departments at Driscoll Children’s Hospital, and the Children’s Hospital of San Antonio, a Christus staff member told STAT.
Christus employees asked to remain anonymous because of emails implying they could lose their jobs for violating the hospital’s “social media policies.”
“Any way you slice it, they’re going to lose money,” said another Christus staff member, who also said that Christus recently offloaded the responsibility for staffing the emergency department to a new private equity-backed joint venture with SCP Health. “I tried to look at all the angles for why they would do it financially, and it just doesn’t make sense. It seems purely ideological.”
That ideology, the staff member said, is a bias against emergency medicine and toward family medicine — the other residency program at Christus Spohn, and the field many of the administrators come from. Staff members who spoke with STAT noted that residency programs are an important tool in bringing physicians to underserved areas where they may stay for their whole careers.
“South Texas is chronically underserved,” a Christus staff member said. “It’d be crazy to say that there’s, any time in the foreseeable future, a surplus of the physicians in this region.”
The future of the emergency medicine work force
In a 2021 presentation about the national surplus predicted by the ACEP study, emergency medicine taskforce members listed various fixes for the problem. These included making residencies four years instead of three in order to decrease the number of graduates; asking programs to adjust the number of available slots in residency programs; asking ACGME to not approve new residency programs, working with CMS to decline funding for new programs in non-teaching or for-profit hospitals; increasing resident salaries; and investigating the legality of for-profit institutions running residency programs.
However, the taskforce acknowledged that the data behind some of these strategies was lacking, and that some of them might be minimally effective, making the path ahead unclear. “Change will take time and precision, yet we must forge ahead as there are no quick fixes for the challenges we face,” ACEP wrote in a brief.
One lever that is currently available for curbing lower-quality residency programs, however, is raising the standards that ACGME uses to certify them. The organization reviews the standards every 10 years, and emergency medicine is expecting the first draft of its readjudication in the next year or so, said Denley.
“This may inadvertently reduce the number of programs or downsize programs if they cannot meet more stringent ACGME standards,” the EMRA wrote in a blog post.
The task force suggested this option too, noting that the number of key procedures a resident currently needs to perform during training is low. For example, emergency residents are only required to perform 35 intubations, but literature suggests “50-60 are needed to achieve competence,” the task force said.
For now, in lieu of a better governance structure for residencies, programs are self-regulating — whether that means opening or closing programs. However, the experts who spoke with STAT emphasized that programs should only be closed with careful consideration from all the stakeholders involved, including the community and the residency program.
In the Christus hospital’s case, staff members told STAT that the decision was entirely made by the hospital administration and presented to them as final. The wife of Christus Shoreline Hospital’s emergency department medical director testified at a Corpus Christi city council meeting on Oct. 17 that her husband hadn’t been involved in a single conversation before the closure decision was handed down.
After several residents spoke against the program’s closure at the meeting, one Corpus Christi city council member addressed another city official.
“You need to have a face-to-face with the [Christus] CEO and find out what the heck’s going on,” he said. “This is not the first time Christus Spohn has made decisions that we had to question, and I think this is a very important [one] we need to get right.”
About the Author Reprints
To submit a correction request, please visit our Contact Us page.











STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect