
An estimated 82,998 people died from opioid overdoses in the U.S. last year. A new study published Friday in JAMA Health Forum drives home how lack of access to lifesaving medications could contribute to these preventable deaths.
The study is the most comprehensive Medicaid analysis of opioid addiction to date, analyzing a national claims dataset with 76 million patient data points between 2016 and 2018. Medicaid patients are already at disproportionate risk of opioid overdoses, almost four times higher than patients on commercial insurance. Correspondingly, Medicaid is one of the primary payers of opioid addiction treatment in the U.S., covering nearly 40% of adults under 65 with this chronic disease.
“It’s a vulnerable slice of the population,” said Elizabeth Armstrong, an assistant professor of social work at the University of Maine, who was not involved with the study. “People’s socioeconomic status, as well as access to secure and stable housing, food security, mental health issues; these are all challenges that tend to cluster together.”
But insurance coverage doesn’t automatically mean that patients have access to treatments like methadone, buprenorphine, or naltrexone — the three FDA-approved medications for treating opioid addiction. Both methadone and buprenorphine activate opioid receptors at safer levels to reduce cravings and are associated with a reduced risk of death. Overall, the study found that 55% of Medicaid enrollees with opioid addiction received some medication treatment nationwide.
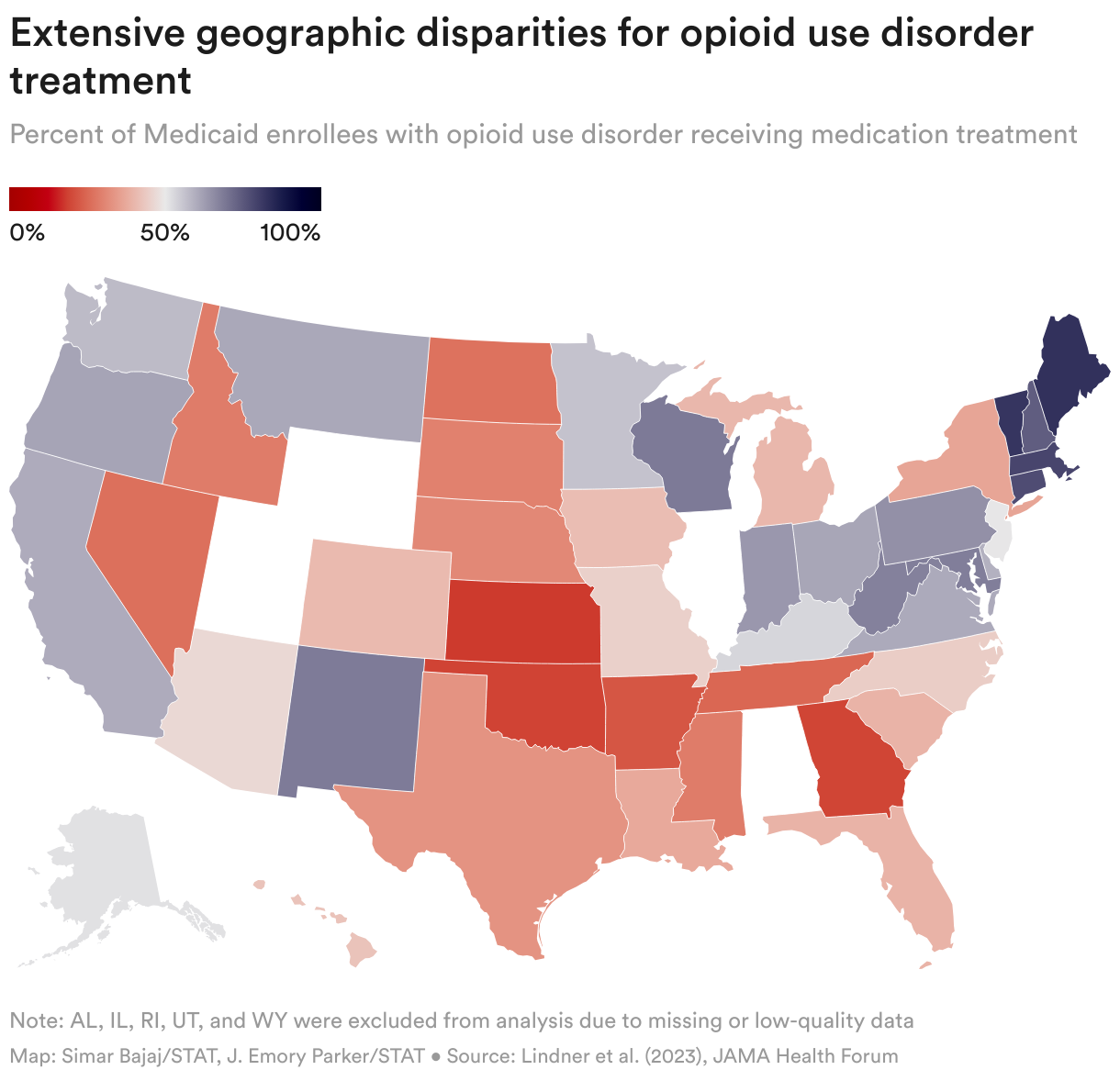
In New England, around 75%-80% of these patients received medication treatment. But in the majority of states in the Midwest and South, fewer than 40% of Medicaid patients diagnosed with opioid addiction received medication. “The variability suggests quality of care problems,” said Dennis McCarty, a study co-author and professor emeritus of public health at Oregon Health and Science University. “It reveals lost opportunities to intervene.”
The authors also revealed significant disparities in treatment access within states. For example, while West Virginia as a whole had an above-average opioid addiction treatment rate of nearly 70%, treatment rates by county ranged from 23% to 82%. Right in the middle was Cabell County with a treatment rate of 64%, infamous for being the epicenter of the opioid epidemic, with 81 million prescription pain pills flooding the region over eight years. In 2018, Cabell County had the highest opioid overdose death rate in the state.
Patrick Marshalek, an associate professor of behavioral medicine and psychiatry at West Virginia University who was not involved with the study, said that while the findings are intriguing, it’s equivalent to “the first shot of a grainy video” — meaning that it’s not yet clear how to interpret some results. For example, across the study period, states varied widely in their coverage of methadone treatment, reimbursement rates, and whether or not they expanded Medicaid under the Affordable Care Act, making it difficult to directly compare state medication rates or extract lessons.
As one example, the study found that 83% of patients with opioid addiction in Maine received medication treatment — the highest rate of any state. But Armstrong thinks this may simply be because Maine hadn’t expanded Medicaid at the time, meaning that the state was insuring a much smaller patient population. “So there may have been less of a disjuncture between the population seeking treatment and the availability of treatment for that study period.”
Health economist Stephan Lindner, the lead author of this study and an associate professor of emergency medicine at Oregon Health and Science University, also noted that the research team wasn’t able to analyze race or ethnicity due to data quality concerns. But given well-known demographic disparities in opioid addiction treatment access, Armstrong suggests that Maine’s relatively homogenous population — about 94% of residents are white — could also help explain the state’s high medication rates.
The most pressing question is what can states do to close treatment disparities. “We fail people by not providing adequate treatment to people with opioid use disorder enrolled in Medicaid,” said Lindner.
Marshalek points to telemedicine as one powerful way to expand access to opioid addiction treatment, especially given that many regulatory barriers were relaxed during the Covid-19 pandemic and may soon become permanent.
Marshalek also said that West Virginia’s hub-and-spoke model serves as an example of how to expand access: Rather than expecting patients to drive hours to the main hospital in order to get medications, experts at WVU’s hub in Morgantown train doctors in primary care clinics and federally qualified health centers across the state to help them distribute opioid addiction treatment within their own communities.
On a similar note, Armstrong recommends providing opioid addiction care within school clinics and expanding access to non-students and family members, given that Medicaid already pays for school-based behavioral health services. In the long term, however, Armstrong says that the U.S. needs more people empowered to provide integrated behavioral health care, which is why she directs the Professional Opioid Workforce Response Program to train social workers in opioid addiction and create a network of providers across Maine.
Lindner also emphasized the need for further research. By using Medicaid claims data, the study is inevitably unable to capture patients who have not interacted with the health care system. “They are flying under the radar, but, very importantly, they’re still there,” said Lindner, “and eventually they’re going to show up in the overdoses.”
Ultimately, combining various streams of data — including Medicaid claims, overdose fatalities, national surveys, and first responder data — could provide greater clarity about the human toll of opioid addiction. From hopelessness to isolation to despair, “there’s a fire burning with this addiction epidemic,” Marshalek said, “and it’s really not that discriminating when it comes to looking for fuel.”
About the Author Reprints
To submit a correction request, please visit our Contact Us page.











STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect